

Temporomandibular disorders (TMD), often less accurately referred to as temporomandibular joint disorders (despite the fact that many conditions within this umbrella term do not affect the joint itself), are very common.
You may also see this referred to as TMJ, though this term refers to the temporomandibular joint itself rather than any associated pathology.
The exact prevalence is difficult to establish as many people with symptoms do not consult a healthcare professional, however studies indicate that approximately 5-10% of the population will be symptomatic to the point of seeking help. One recent review has concluded an overall prevalence as high as 31% however.
TMD symptoms are something that may be discussed in a tinnitus consultation, particularly if patients complain of symptoms other than classical tinnitus. Indeed asynchronous and non pulsatile tinnitus is often subjective, with the specific term “somatosensory tinnitus” being ascribed to tinnitus in the context of a neck injury or TMD.
A number of otologic symptoms appear to be more commonly reported by patients with TMD, including ear fullness, otalgia(ear pain), vertigo, hearing loss and tinnitus.
However, the evidence base for the association with tinnitus is regarded as poor and contentious, being predicated on series of published cases or small cohorts of patients. Whilst there is an association between the two problems, cause and effect has proved harder to establish!
That said, the proportion of TMD patients with tinnitus specifically can be quite high, with figures reported anywhere up to 70%.
In addition, there is some low-level evidence attesting that conservative and reversible TMJ treatment strategies may improve patients’ experiences of co-existing tinnitus.
Often what is felt as “ear pain” is really referred pain (i.e. originating from) other structures close by, including the TMJ, due to the shared sensory supply between these areas and the ear. In fact, the jaw and middle ear share an interesting developmental origin.
Oto presents the essential facts on what TMD means, the different types of problems under this umbrella, how they may co-exist with tinnitus, and some suggestions for how they can be treated.
What is the Temporo-Mandibular Joint (TMJ)?
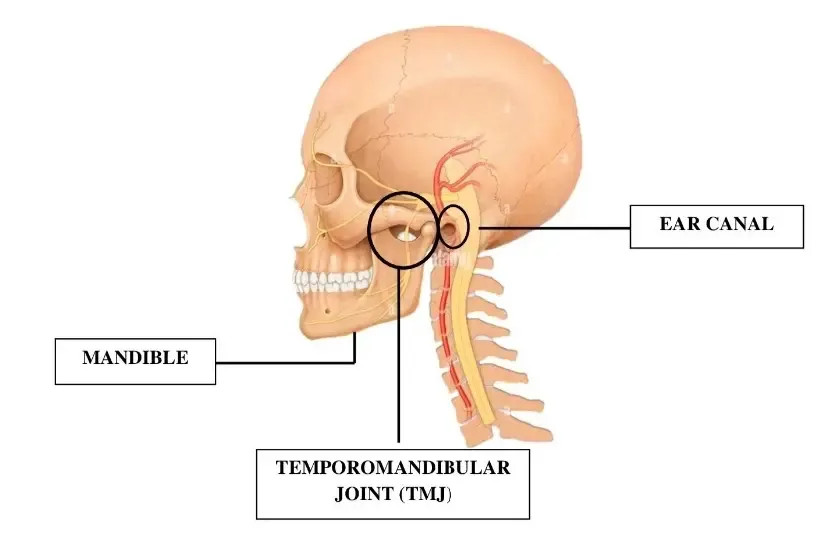
What is the TMJ, anyway? The temporomandibular joint is surprisingly complex, allowing opening and closing of the mouth as well as side to side movement.
The joint itself connects the jaw (mandible) to the skull (at the temporal portion). The joint works with muscles to allow chewing, yawning, swallowing, and talking.
The TMJ is unique in being “ginglymoarthroidal” – that is its action is a combination of rotation (the initial phase of mouth opening) and sliding or translation (achieving full mouth opening).
In addition, the two joints on either side of the head function in tandem to work as a team and enable function.
What Are Symptoms Of TMD Disorder?
TMD is an umbrella term that can encompass problems affecting the TMJs themselves, as well as the associated muscles of mastication (chewing muscles). A disorder occurs when the normal physiology and function of the TMJ or associated structures is impaired.
Most commonly, people seek help with TMD when they experience symptoms that may be related, such as:
- Pain at, or near, the TMJ, including at the ear;
- “Clicking”, “popping”, “grinding”, or other noises in the ear;
- Restriction of mouth opening (trismus);
- Limitation of dietary choices (particularly the need to avoid hard or chewy foods);
- Headaches and/or associated neck pain;
- Clenching or grinding teeth.
Patients may also be referred to a clinician with a sub-specialist interest in TMD by colleagues in otorhinolaryngology (ENT surgery) with unexplained symptoms including otalgia, ear fullness and tinnitus that have not been confidently ascribed to an alternative cause.
It is important to remember that as TMDs are very common and many of these symptoms are non-specific and may have many causes, the experience of one or more of these does not mean that the person definitely has a TMD.
Indeed over a third of the population may manifest at least one symptom and painless clicking at the joint is particularly common (and requires no treatment!).
Ear And Jaw Pain

Ear and jaw pain are easy to confuse due to referred pain, or there might be a true cause to having both ear and jaw pain. Either way, seeking medical advice is important so that a proper diagnosis can be established and suitable treatment can be recommended.
When ear pain accompanies jaw pain due to TMD, you may find relief from resting the jaw, eating soft foods, using warm compresses or ice packs, and using pain relief as required. Additionally, targeted physical therapy exercises may be effective in reducing jaw pain.
Medications prescribed may include non-steroidal anti-inflammatory drugs (NSAIDs), opioids, muscle relaxants, tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs) and serotonin and noradrenaline reuptake inhibitors (SNRIs) among others.
Sometimes ear and jaw pain are accompanied by other symptoms such as noise in the ear, especially when the jaw moves. The sounds in the ear can arise from fluid in the middle ear as well as intra-articular TMJ problems, so it's important to seek proper diagnosis by a medical professional.
Noises from the TMD: what do they signify?
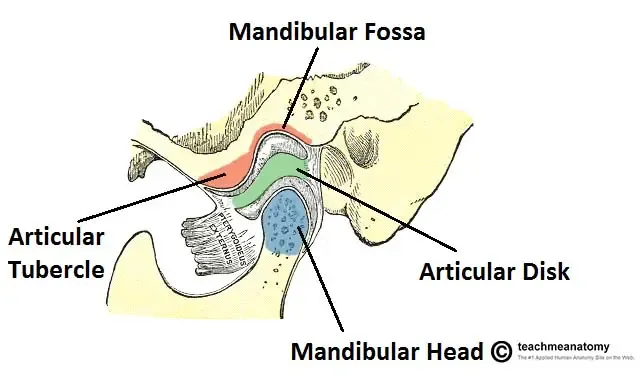
A common complaint of people with TMDs is noise in the ear, including “clicking” or"crunching" sounds. Clicking most commonly results from a displacement of the meniscus or articular disc, which is a fibrocartilage disc interposed between the surfaces of the joint.
The disc “slips forwards” in some people (anterior disc displacement) and is then “recaptured” on full mouth opening, resulting in a “click”.
This can be painful, as whilst the disc centrally has no innervation, the back of the disc (retrodiscal tissue) is richly supplied with sensory nerves. Disorders, where the disc is displaced, may be collectively referred to as “internal joint derangement”.
A “crunching” noise in the ear can also be due to fluid in the middle ear (i.e. otitis media) or due to ear wax. Ear wax may cause obstruction or near-complete obstruction of the ear canal, and may in turn be affected by the movement of the jaw.
Ear wax should be managed or removed by a professional such as an otolaryngologist, general practitioner, or audiologist. Fluid in the middle ear may resolve on its own, or a physician may prescribe medication with the aim of helping the fluid clear up more quickly.
Degenerative damage to the TMJ can occur due to arthritis, which may be secondary to systemic causes. “Crunching” or crepitus may also be an indicator of more advanced degenerative changes, including various types of arthritis (e.g. osteoarthritis, rheumatoid arthritis, psoriatic arthritis, etc.).
Some people don't hear a noise but rather report that the ear “feels full” or “clogged”. Of note, ear “fullness” or a “clogged” sensation can be a symptom of ear wax or hearing loss due to a variety of causes. Both ear-wax and hearing loss can precipitate and/or aggravate tinnitus.
If the hearing loss is permanent, hearing aids can be helpful in addressing both tinnitus and hearing loss.
Is there a relationship between TMD and tinnitus?
As discussed in the introduction, there is quite a bit of low-level evidence for the association between TMD and tinnitus, although no clear cause and effect relationship, and the link is contentious.
The earliest reports of an association date back to 1934 when a man called Costen published cases presenting with the two conditions combined, earning it the nickname Costen’s syndrome.
Many publications have since followed and, along with these, an almost equal number of anatomical theories as to why the two problems might be seen together more frequently than chance would seem to dictate.
These theories have included excessive pressure on nerves (e.g. the chorda tympani), stretch on muscles (e.g. the tensorveli palatini muscle), and ligaments (e.g. the sphenomandibular ligament), as well as central mediation theories involving structures in the brain.
Again there are a number of studies showing that TMD may be associated with symptoms as diverse as vertigo, hearing loss, and pruritus (itchiness) of the ear canal, although the cause and effect relationship is difficult to establish.
How Long Does TMD Last?
TMD can be acute (lasting days to weeks) or chronic. How long it may last depends on many factors, including the underlying cause, as well as the classification of the TMD.
There are a number of classification systems in use, but broadly speaking one can classify problems as:
- Myofascial pain: whereby pain predominantly affects the muscles of mastication around the joint, potentially as a result of overuse and/or parafunctional habits such as grinding, clenching, biting nails, chewing gum, etc.;
- Internal derangement of the joint: as noted due to a displacement of the articular disc which may be an incidental finding in a much larger proportion of the (asymptomatic) population;
- Degenerative joint disease: effectively arthritis which may be “wear and tear”(osteoarthritis) or inflammatory (e.g. rheumatoid, psoriatic, etc.).
The sooner the nature of the TMD is diagnosed, the sooner treatment can commence and relief can occur. It is important to note that there may be an element of psychosocial issues, also known as “functional overlay”, whereby symptoms can be precipitated or aggravated due to co-existing mental health problems such as depression and anxiety.
The overlap between myofascial pain, internal joint derangement, degenerative joint disease, and psychosocial issues is far from clear-cut and multiple pathologies may be responsible for the presentation in a single patient.
How is TMD diagnosed?

It may take multiple modalities to diagnose and treat TMD, and your medical professional will determine which modalities are appropriate. The initial diagnosis is often clinical and based on a combination of the history (the “story” of your symptoms) and the examination findings.
This is augmented with a number of reproducible measurements such as self-reported pain scores, dietary scores, quality of life questionnaires, and measurements (e.g. interincisal distance, protrusive and lateral excursions).
A number of imaging modalities may also be recommended:
- An orthopantomogram (OPG) plain film radiograph: this serves as a “screening tool” which is readily available, has a low radiation dose, and can often exclude severe changes to the joint and significant worrying pathologies, as well as ruling out dental causes for any pain;
- A computed tomography (CT) scan: this is used to look at the hard tissues of the joint and is often the chosen investigation where advanced degenerative changes are suspected either clinically or on the plain film radiograph;
- A magnetic resonance imaging (MRI) scan: this is often good at demonstrating the soft tissues of the joint including the articular disc, although the reporting Radiologist may “overcall” and “undercall” things as the correlation with arthroscopic and surgical findings is not always straightforward.
There can be multiple contributory factors to symptomatic TMDs developing. These can include:
- Joint overloading and cumulative “microtrauma” from habits (e.g. chewing gum) and parafunction (e.g. bruxism, clenching);
- Systemic illnesses, especially inflammatory arthropathies;
- Direct traumatic injury to the joint (“macrotrauma");
- Psychosocial factors;
- Indirect trauma (e.g. transmitted forces from intubation, dental extractions, or lengthy dental procedures).
What can be done about TMD?

There's good news about TMDs as many patients will find their problems self-resolve and over 80% of patients seen with TMD in secondary care will settle with conservative management. Conservative treatment usually includes reassurance, patient education, a soft diet, resting the TMJ and surrounding area and using warm compresses and/or ice packs.
Topical NSAIDs can provide an excellent low-risk pain management strategy (e.g. ibuprofen 5% gel) but other painkillers may be required. TMJ physiotherapy can also be used and this can be done under the guidance of a physiotherapist (ideally one registered with the ACPTMD or Association of Chartered Physiotherapists in Temporomandibular Disorders) as it is valuable to see someone with a specific interest in the condition.
In the absence of acute inflammation, a self-directed exercise program can be equally beneficial. There are many treatments for TMD but the right combination of treatments depends on the cause of the TMD and the individual patient's needs.
For patients refractory to conservative management, other options may include:
- An occlusal “splint” or bite-raising appliance;
- Prescribed medication;
- Acupuncture;
- Cognitive behavioural therapy (CBT)
- Intra-articular injections e.g. steroids such as Depo-Medrone®;
- Botulinum toxin injections (e.g. Botox®, Dysport®);
- Arthrocentesis or a “wash out” of the TMJ;
- Arthroscopy of the TMJ (using a small camera and instruments to perform minimally invasive surgery to the joint);
- Open surgery (arthroplasty) including reshaping the joint and/or repair or removal of a damaged disc (meniscectomy);
- Total prosthetic replacement of the TMJ.
For more information on the surgical options please visit Elledge Surgical.
Join Oto
The Oto app may soothe TMD-related symptoms with resources such as CBT for tinnitus, guided meditation to reduce stress, sound enrichment, and physical therapy exercises for the jaw, tongue, and neck/back:
- Neck stretch stretches the neck in multiple planes for improved flexibility and relaxation.
- Neck and shoulder release is a quick exercise that encourages awareness and release of tension in the neck and shoulders.
- Shoulder rolls loosen and relax tension in the neck and shoulders.
- Tongue stretch engages the muscles of the mouth and jaw.
- Arm swing releases tension in the shoulders, arms, and hands by swinging arms in opposition front and back.
- Deeper neck stretch thoroughly engages the muscles, tendons, and ligaments of the neck for sustained relief.
- Gentle neck rotation increases neck flexibility.
- Shoulder stretch increases the flexibility of the shoulder muscles.
Check out Oto's Tinnitus Support Group, a supportive community for individuals with tinnitus or related conditions to receive regular tips and tricks from the expert team at Oto!
FAQs
What is the difference between TMD and TMJ?
TMD refers to Temporomandibular Disorders, which encompass various conditions affecting the temporomandibular joint and surrounding structures. TMJ, on the other hand, specifically refers to the temporomandibular joint itself.
How prevalent is TMD?
TMD is quite common, with studies indicating that approximately 5-10% of the population will seek help due to symptoms. Some reviews even suggest a prevalence as high as 31%.
How is tinnitus linked to TMD?
Tinnitus can be associated with TMD. Patients with TMD can report symptoms such as ear fullness, ear pain, vertigo, hearing loss, and tinnitus. However, the exact cause-and-effect relationship between the two is unclear and remains a topic of debate.
What are the common symptoms of TMD?
Symptoms of TMD can include pain near the TMJ or ear, noises like clicking or grinding in the ear, restricted mouth opening, dietary limitations, headaches, neck pain, and habits like teeth clenching or grinding.
How is TMD diagnosed?
Diagnosis of TMD is often based on clinical findings, patient history, and examination results. Imaging modalities like orthopantomogram (OPG), computed tomography (CT) scans, and magnetic resonance imaging (MRI) can also be used for a more detailed assessment.
What treatments are available for TMD?
Conservative treatments for TMD include patient education, a soft diet, resting the TMJ, warm compresses, ice packs, and pain management strategies like topical NSAIDs. More advanced treatments can range from occlusal splints, prescribed medications and, in certain situations, surgical interventions.
Can the Oto app help with TMD-related symptoms?
Yes, the Oto app offers resources such as CBT for tinnitus, guided meditation, sound enrichment, and physical therapy exercises targeting the jaw, tongue, neck, and back to help alleviate TMD-related symptoms.